EMIS Web - Recording of Domestic Abuse and MARAC information on Electronic Medical Records (EMR)
Relevant Principles
All recording of domestic abuse information
- ALL information in the EMR (Electronic Medical Record) about domestic abuse MUST be hidden before saving a consultation from Patient Online Access. All added information can be seen immediately from online access unless hidden.
- Family records should be linked in practices where possible.
- The name of anyone accompanying a patient in a consultation should be documented.
- The name of any alleged perpetrator/s should be included when documenting disclosure of DA.
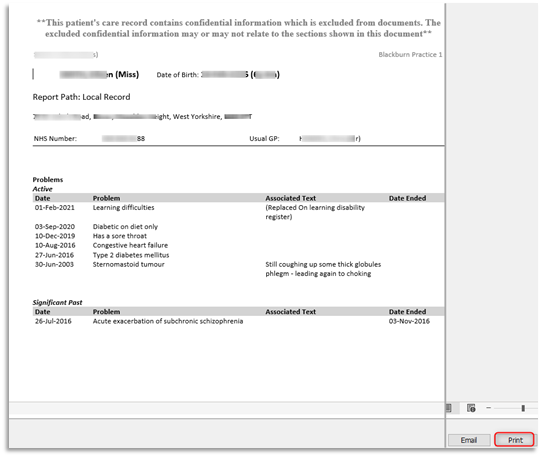
- Ensure that any reference to DA on a victim’s records is not accidently visible to the perpetrator during appointments. The computer screen showing the medical record should never be seen by third parties (i.e. family or friends accompanying a patient). When providing a summary printout for a hospital admission for example, care should be taken that information about DA is not inappropriately included when printing out these summaries to give to patients as the perpetrator may see this. Please remember that when a Full/Brief Summary is printed off from a patient record everything will be included. Therefore Summaries will need checking and any information about domestic abuse must be redacted.
- Never disclose any allegation to the perpetrator or other family members.
- Ensure that any decision to record the information in the perpetrator’s EMR is made with due regard to the associated risks.
- Ensure that any reference to DA in a perpetrator’s record is redacted if provided to the perpetrator unless you are certain it is information that the perpetrator already knows. For example, the perpetrator has disclosed this information themselves to you, or there is a relevant conviction which the perpetrator has disclosed or is aware has been disclosed to you such as in Child Protection Conference minutes when the perpetrator has been present at the conference and is aware this information is being shared.
- Be aware of the potential danger of the perpetrator having access to information about their abuse and to information in children's EMRs; this includes via online access to their own information and their children’s information, as well as coercive access to the victim’s EMR.
- If you are not sure whether someone is a victim or perpetrator of abuse, or there is suggestion or evidence that someone is both, we recommend following the guidance on documenting victimisation.
Subject Access Requests
Information about third parties and information that may cause serious harm to either the patient or others should be redacted. For example, ensure that any reference to DA/MARAC is redacted from children’s records if provided to the perpetrator.
Recording disclosures
Domestic abuse (victim)
1.0 Victim Record
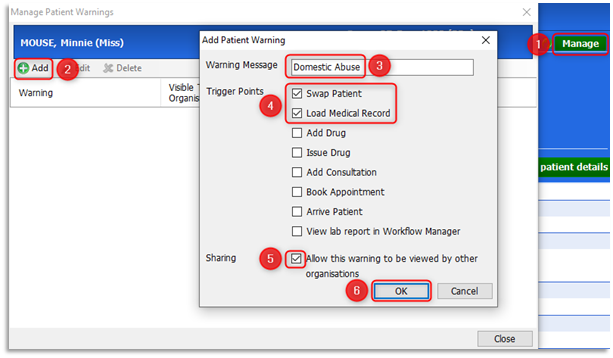
1.1 If a patient discloses domestic abuse, record this information within the Patient Warnings section of the patient record in free text. In Emis with the patient active, double-click on the Precis bar (blue demographic bar) to open it. Select Manage and from the Manage Patient Warning screen click Add. In the Warning Message Field enter the text and select (tick) all the relevant Trigger Points. Finally select Allow this warning to be viewed by other organisations and click OK:
1.2 The following warning will appear every time the care record loads and a consultation is added for the patient:
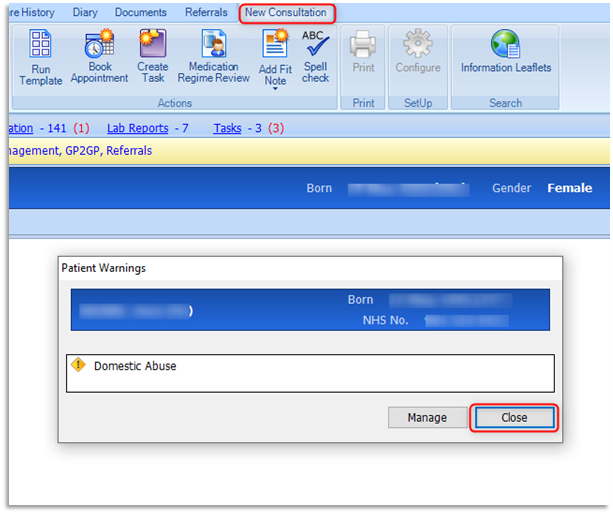
1.3 The clinician will view the warning and select Close.
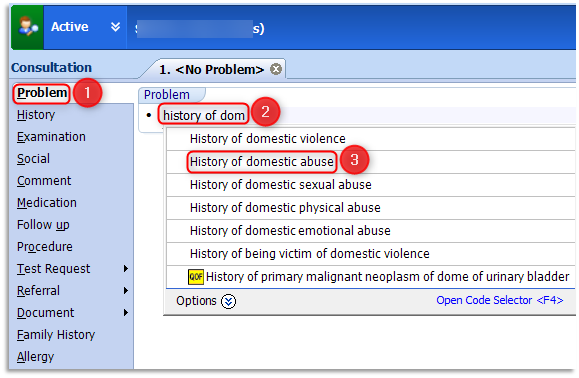
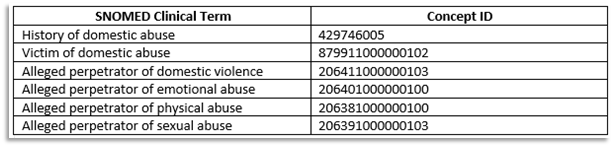
1.4 Record the disclosure in the main body of the patient care record (under a Problem heading within a Consultation). With a new consultation open, click once on the Problem heading, with the cursor flashing start typing the relevant clinical term i.e.: History of domestic abuse or Victim of domestic abuse etc. As you enter the text the related terms/codes will appear within the pick list. Double-click the relevant term from the available list:
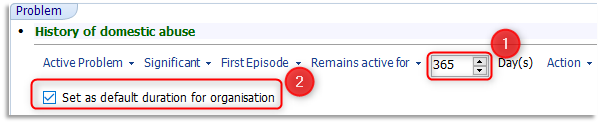
1.5 This following example shows the selection of 'History of domestic abuse'. On selection the problem defaults to Significant and will remain an active problem for the default 84 days:

1.6 The length of time to be stored on the list of active problems should be requested by the clinician when inputting this information. The clinician can change the default setting for the practice from 84 days to a more suitable timeframe of 365 days, for this and any future recordings of History of Domestic Abuse. Click into the Day(s) active field and enter 365 and place a tick in the Set as default duration for organisation:
1.7 Click once on the Comment Heading and with the cursor flashing enter free text to include what the patient has said in their own words and any relevant information:

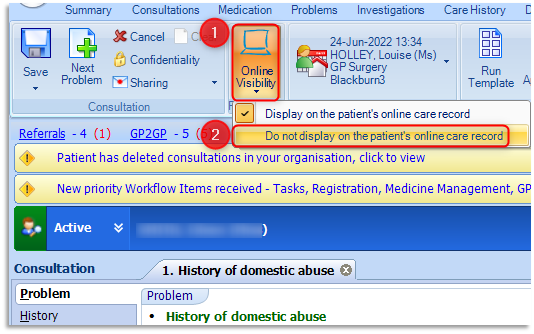
1.8 The clinician can request that this consultation and problem is stored as Do not display on the patient’s online care record, so that it will not be visible if a patient requests to see their records online. This option is available whilst a clinician is adding a consultation by selecting Online Visibility option on the ribbon and then selecting Do not display on the patient's online care record:
1.9 Click Save on the ribbon to save the consultation. This problem will automatically be added to the 'Active' Problems of the patient's care record for the required duration. After the set time the problem moves to 'Significant Past' history of the Problems tab of the care record.
1.10 Online visibility can also be added to a consultation in retrospect, i.e. hidden from online access after a consultation has been made. To do this right click on the required consultation entry (blue header) as shown below and select Online visibility from the available options, then select Do not display on the patient's online care record:

1.11 Any consultations that have been hidden from online visibility will be indicated by a computer icon with a red cross:

1.12 Please note: If the patient moves to another surgery, the electronic information will be visible in the list of Problems and Consultations but Patient Warnings information will not be transferred.
Child/Vulnerable Adult
(within the household record)
1.13 Add to the record following the same procedure as above, including online visibility protection.
Perpetrator record
1.14 If an adult victim/child discloses domestic abuse, ensure the perpetrator record is linked to the record of the victim, any children or any vulnerable adults within the household. Do not record the disclosure in the alleged perpetrator record unless your professional judgement deems it necessary. Apply online visibility protection if any information is recorded, as previously demonstrated 1.10 of this document.
Child Disclosure
2.0 If a child discloses domestic abuse follow the same procedure as for when a victim discloses domestic abuse in Section 1.0. Add to the non abusing parent record and to any sibling/vulnerable adult within the household records. Ensure the perpetrator’s record is linked to the record of the victim, any children or any vulnerable adults within the household.
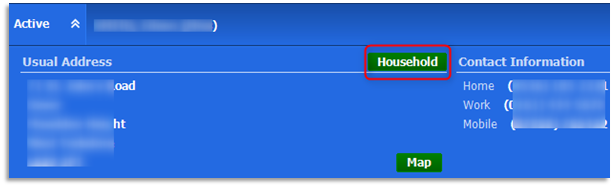
2.1 Double-click the patient's Precis bar and click on the Household button to check for other household members registered (Active) at the practice. This link is entirely dependant on the same household (address) being recorded against all family members' registration details:
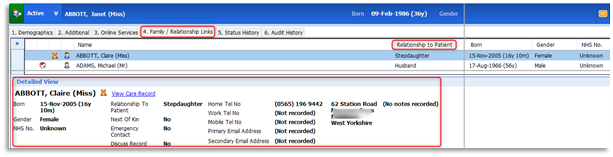
2.2 An addition to the Household button, family members can be added to Family/Relationship Links section of a patient's registration details. Please note that this is not an automatic link and must be added manually for each patient. With the relevant patient selected click on the Registration icon. Select option 4: Family / Relationship Links tab. Add a relationship using the Add Relationship button on the ribbon, completing all the necessary details and click OK. All family members' details can be added, including individual relationships to the selected patient. Highlight each family member to view their details in the lower pane:
2.3 Do not record in the perpetrator record unless your professional judgement deems it necessary. Ensure online visibility protection is applied.
Perpetrator Disclosure
2.4 If a patient discloses that they are a perpetrator of domestic abuse add these details in free text to the Patient Warnings. Record the disclosure in the main body of the record (within the Problems section of Consultation) – include what the patient has said in their own words and any relevant information. Add the relevant code – ‘Alleged Perpetrator of Domestic Violence’, this will automatically be added to the 'Active' Problems of the care record.

2.5 Use the online visibility protection to hide this consultation from online access before saving the consultation.
Adult Victim, Children or Vulnerable Adult Record (When disclosure made by perpetrator)
2.6 If a patient has disclosed that they are a perpetrator of domestic abuse, add the disclosure (code: History of Domestic Abuse) to the consultation page in the adult/child victim's care record, as stated in Section 1.0 above ensuring online visibility protection is applied before saving the consultation.
MARAC
Information shared with Multi Agency Risk Assessment Conferences (MARAC’s) – Including any referral made to MARAC/requests from MARAC for information and information shared with the MARAC:
Records of Adult Victim, Children and Vulnerable adults in the household who are subjects of MARAC
2.7 Referrals to MARAC and requests for information from MARAC and information sent to MARAC could be in the form of a telephone consultation or via email as an attached document. If received by telephone, add a telephone consultation and record 'Subject of multi-agency assessment conference' as a Problem within the consultation entry. Enter any relevant history or comments and hide from online visibility before saving the consultation as shown in 1.4-1.9.
2.8 If referrals are received via email, on attaching or scanning the referral document into a patient's care record either option will prompt the following fields to be entered:
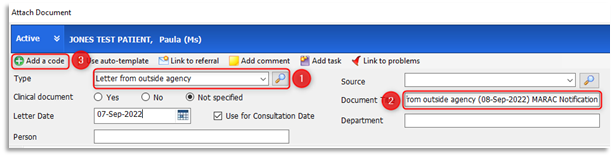
2.9 Select a document Type of 'Letter from outside agency' using the browse icon as shown above at point 1, enter the term 'letter from outside agency' from the code selector field double-click the relevant term to select it. Click into the Document Title field at point 2 and type 'MARAC Notification'. The Document Title accompanies the attachment (paperclip icon) and is clearly visible within the Consultations tab as well as the Documents and Care History tabs of the patient's care record. Record the date on the document and select Use for Consultation Date, this option will ensure that the consultation will be filed against the letter date selected. Click on Add a code to add the following code/term in the Code Selector field: 'Subject of multi-agency risk assessment conference':

2.10 Select the relevant term and click OK. Ensure that the 'Record as Problem' check box is selected. Select a suitable timeframe that the problem will remain active for (set for the entire organisation if required) and click OK. Click File to save to the patient's care record and hide from online visibility as shown in Section 1.10. Ensure that any reference to MARAC/DA is redacted from the record for a Subject Access Request and ensure that any reference to MARAC/DA is redacted from children’s/vulnerable adult's records if provided to the perpetrator.
Alleged Perpetrator subject of MARAC
2.11 An alleged perpetrator subject of MARAC is not informed that the MARAC is taking place. GP Practices must never share information related to MARAC with an alleged perpetrator as doing so could be dangerous to the victim and will likely increase risk to the victim. Any request for information for the MARAC received by the Practice and any record of information sent to MARAC by the Practice should be scanned into the record and protected from online visibility. Do not apply any codes related to domestic abuse or MARAC.
Feedback received from Multi Agency Risk Assessment Conferences (MARACs):
Record of Adult Victim, Children or Vulnerable Adult in the household.
2.12 Scan or attach the MARAC feedback report into EMR using the code Subject of multiagency risk assessment conference and add a Significant Active Problem of History of domestic abuse within the consultation record.
2.13 Use the online visibility function to hide this report and this consultation from patient online access. Ensure that any reference to DA/MARAC is redacted from the record for a Subject Access Request and ensure that any reference to MARAC/DA is redacted from children’s/vulnerable adult's records if provided to the perpetrator.
Record of alleged Perpetrator
2.14 If the Practice receives feedback from MARAC related to the perpetrator this information must never be shared with the perpetrator. The RCGP recommends that no information from MARAC should be stored in the perpetrator's record due to potential risk of being seen by the perpetrator. However if the GP in their professional judgement feels that it is necessary to store the information received, then any information that is scanned in or attached should be protected from online visibility before saving and redacted from any Subject Access Requests or summary printouts.
2.15 GP Practices must protect information regarding domestic abuse from the perpetrator. If any requests are made by a named perpetrator to see GP records or the records of their children, the practice must take care in redacting any information relating to the victim, children or the MARAC. GP practices should never inform the perpetrator that a MARAC is/has taken place. GPs can apply physical screen privacy filters to prevent a patient seeing sensitive information during a consultation:
 A physical screen privacy filter
A physical screen privacy filter
2.16 GP Practices must also be aware that perpetrators of domestic abuse may use coercive control to access the medical records of victims and children online. If this is a concern this should be discussed with the victim and the decision can be made to either exclude from online access or if there are concerns that doing so would raise suspicion and increase risk to the victim, consultations and entries related to domestic abuse and MARAC can be hidden.
2.17 Any flag/alert on a record relating to MARAC should remain on the record for 1 year post MARAC.
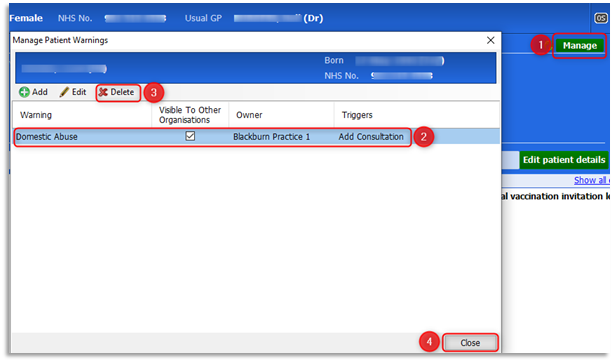
2.18 To remove information added to a Patient Warning, double-click on the patient's Precis bar to open/expand it and click on Manage, then highlight to required warning entry and select Delete, then click OK:
Summary Printout Guidance
3.0 As detailed in the Principles at the beginning of the guidelines, all Summary printouts (Full or Brief) will not redact information that has been hidden from online visibility. Please ensure to follow the recommended next steps to print out care record content and redact sensitive information using a User Defined Summary.
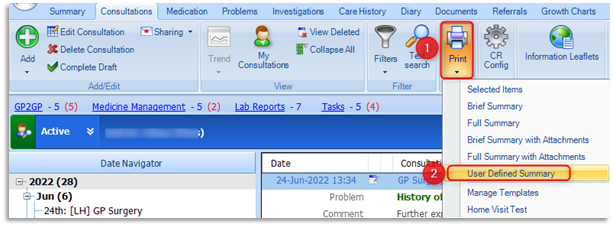
3.1 A User Defined Summary can be printed from multiple tabs within the care record. This example is demonstrating from the Consultations tab. Select the Print option on the ribbon and only choose User Defined Summary:
3.2 The Demographics tick box will be pre-populated. Select/tick the relevant items for inclusion in the print out. Do not select Problems as sensitive problems cannot be redacted!:
3.3 Select/tick Consultations to include them and then click on the Filter (last 3 consultations):
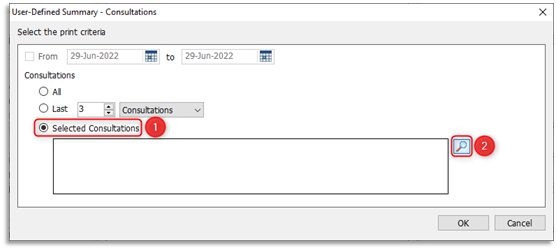
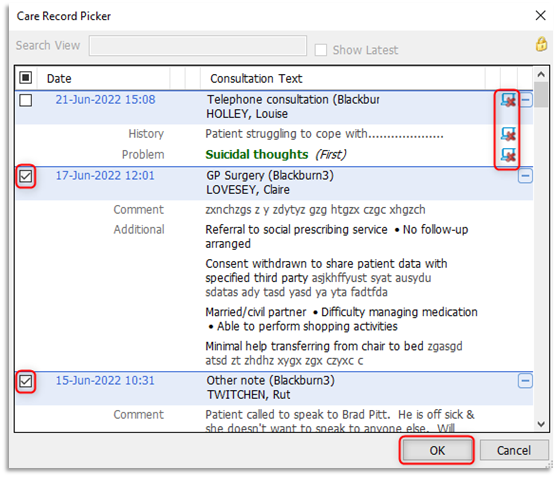
3.4 From the print criteria window click Selected Consultations, then click on the browse (looking glass) icon. At the Care Record Picker all consultations, including those that are hidden from online visibility, will be displayed. Give careful consideration before selecting/ticking the consultations that are to be included in the print out. Please note: unticked/deselected consultations will not be included in the print out, Click OK:
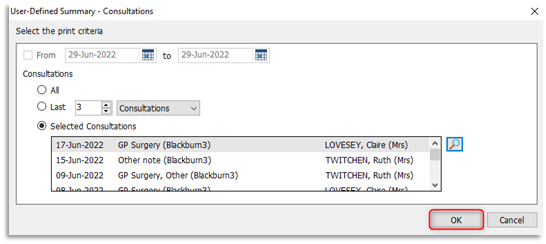
3.5 At the print criteria window a list of the selected consultations will be displayed, click OK:
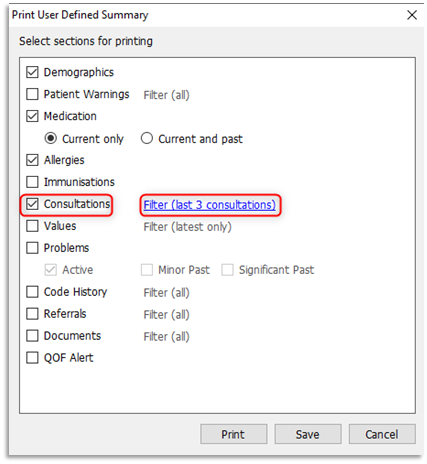
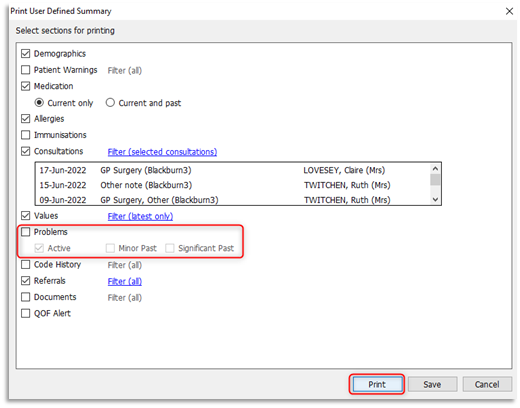
3.6 At the Print User Defined Summary window ensure the Problems tick box is not selected and click Print:
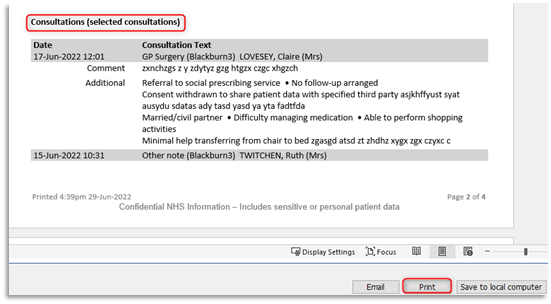
3.7 The User Defined Summary will be viewable detailing all the selected items. Please view the document's content before clicking on Print:
3.8 To include the problems that were omitted from the User Defined Summary, click on the Problems tab of the care record:
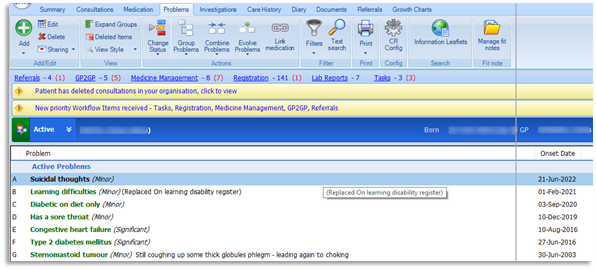
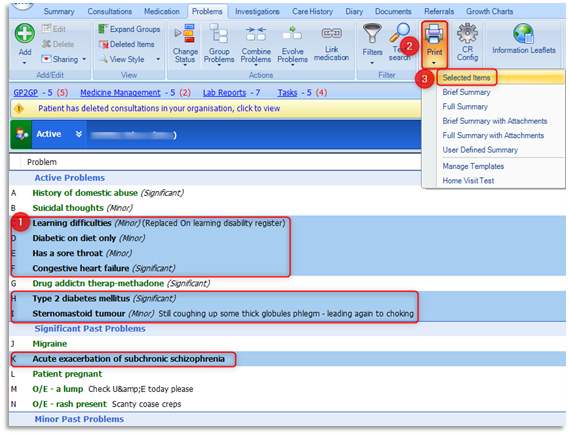
3.9 Carefully highlight (select) the required problems for inclusion in the print out by either typing on the keyboard the adjacent alphabetical letters (i.e. A, B, C etc.) or by holding down the Ctrl Key on the keyboard and individually clicking on the required problem items. The included problems will be highlighted in blue. Click on Print on the ribbon and then choose Selected Items:
3.10 A report containing the patient's demographic information and a list of the selected problems will be displayed. Click Print and attach this document to the previously printed User Defined Summary: